
When Treatment Affects Intimacy
Recognizing and Managing Medication-Associated Sexual Dysfunction in People with IDD
By Mary Pittaway, MA, RDN
Summary: Sexual dysfunction is a common but frequently overlooked adverse effect of psychotropic and other commonly prescribed medications. In men with intellectual and developmental disabilities (IDD), identification can be particularly challenging because symptoms may not be verbally reported and may instead present as behavioral changes, reduced interest in sexual activity, frustration, or changes in mood. In addition, polypharmacy is common in this population and may increase the likelihood of medication-related sexual side effects. Routine screening for sexual health concerns should be considered during medication reviews, particularly when selective serotonin reuptake inhibitors (SSRIs), antipsychotics, opioids, or other high-risk medications are prescribed.

Sexual dysfunction is a common but frequently overlooked adverse effect of psychotropic and other commonly prescribed medications. In men with intellectual and developmental disabilities (IDD), identification can be particularly challenging because symptoms may not be verbally reported and may instead present as behavioral changes, reduced interest in sexual activity, frustration, or changes in mood. In addition, polypharmacy is common in this population and may increase the likelihood of medication-related sexual side effects. Routine screening for sexual health concerns should be considered during medication reviews, particularly when selective serotonin reuptake inhibitors (SSRIs), antipsychotics, opioids, or other high-risk medications are prescribed.
Common Presentations of Sexual Dysfunction
Medication-related sexual dysfunction may include:
Inability to achieve orgasm (anorgasmia)
Delayed orgasm
Delayed ejaculation
Reduced sexual pleasure
Decreased libido (sexual desire)
Erectile dysfunction
Challenges Specific to Individuals with IDD
Sexual side effects may be difficult to recognize because:
Communication differences may limit symptom reporting.
Symptoms may be expressed through behavioral changes rather than verbal complaints.
Sexual health is not routinely discussed during clinical encounters.
Multiple medications may contribute additive sexual side effects.
Clinicians should consider medication-related sexual dysfunction when new behavioral concerns emerge without another clear explanation.
Medications Most Frequently Associated with Sexual Dysfunction
Among men with IDD, SSRIs and antipsychotic medications are the most common medication-related causes of inability to reach orgasm during masturbation or partnered sexual activity.
Relative Risk of Sexual Dysfunction
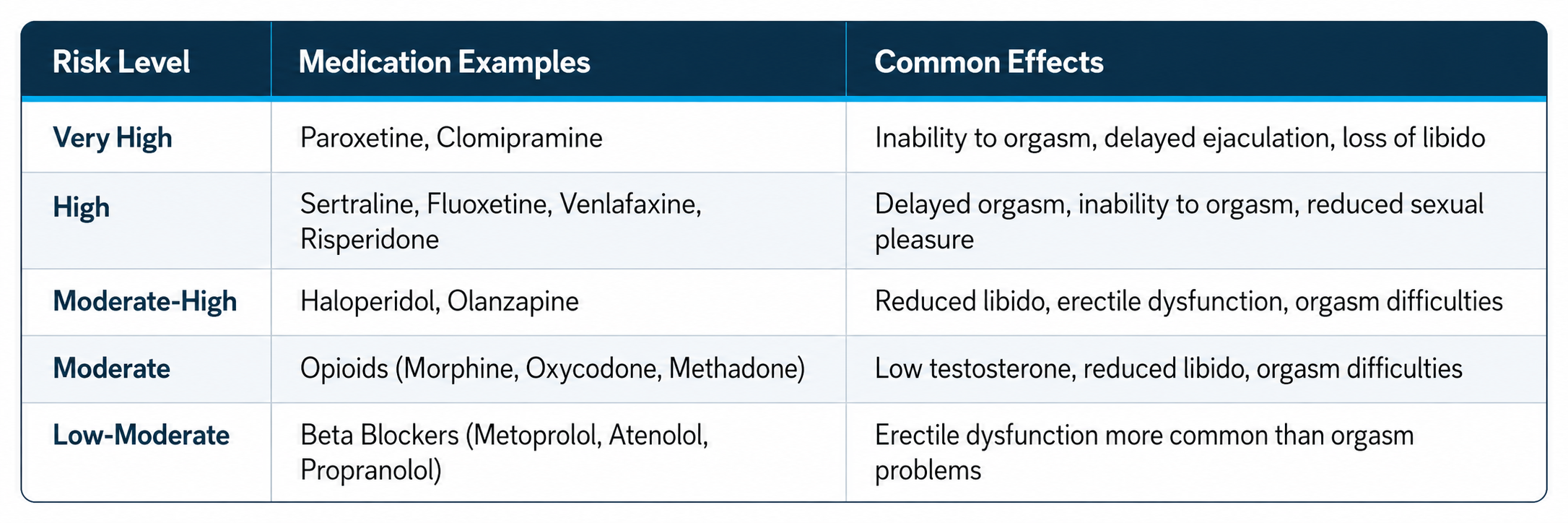
Medications Most Commonly Associated with Inability to Orgasm
Paroxetine
Clomipramine
Sertraline
Fluoxetine
Venlafaxine
Risperidone
Haloperidol
Clinical Assessment Recommendations
When evaluating possible medication-related sexual dysfunction:
Review current medications, including recent dose changes.
Ask direct but respectful questions regarding libido, erections, ejaculation, and orgasm.
Consider whether symptoms began after medication initiation or dose escalation.
Evaluate for contributing medical conditions, including:
Diabetes
Cardiovascular disease
Hypogonadism
Depression or anxiety
Substance use
Consider laboratory evaluation when indicated, including testosterone and vitamin D levels.
Sexual hypersexuality use of Depot medroxyprogesterone acetate (Depo-Provera) when prescribed for males with IDD, it is typically in highly specialized circumstances to reduce severe hypersexuality or sexually disinhibited or harmful behaviors that cannot be managed with behavioral interventions or other medications. Its use is off-label in this population and is generally reserved for cases requiring testosterone suppression, as it can significantly reduce libido and sexual drive but is also associated with important adverse effects including hypogonadism, erectile dysfunction, mood changes, and bone density loss.
Vitamin D and Sexual Function
Evidence from studies in the general male population suggests that low vitamin D levels may be associated with:
Increased severity of erectile dysfunction
Reduced testosterone levels (in some studies)
Impaired endothelial and vascular function
Potential mechanisms include effects on:
Nitric oxide pathways involved in erectile function
Testosterone regulation
Overall vascular health
Although observational studies demonstrate an association between vitamin D deficiency and erectile dysfunction, a direct causal relationship has not been definitively established.
Medications in Women with IDD Associated With Sexual Dysfunction
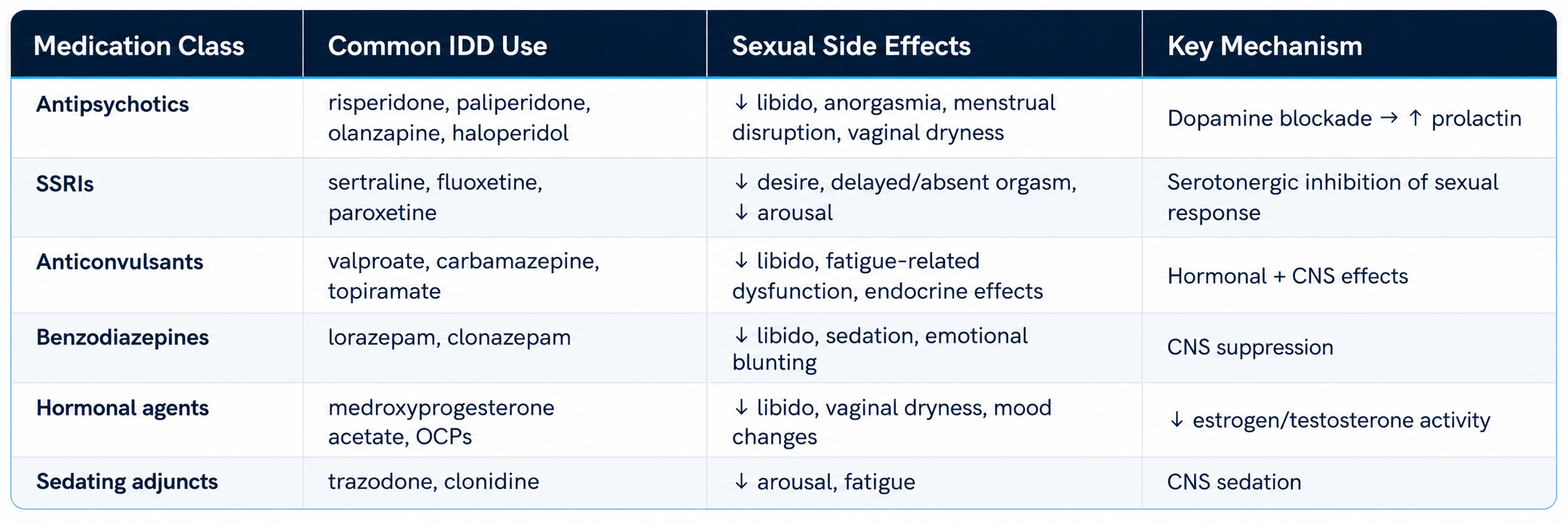
Female IDD-Specific Risk Pattern
Women with IDD are disproportionately exposed to:
Antipsychotics + SSRIs + anticonvulsants (polypharmacy)
Long-term sedatives (PRN → chronic use)
Hormonal suppression for menstrual management
Polypharmacy Effects (IDD-relevant)
Additive sedation → global loss of sexual interest
Antipsychotic + SSRI → highest dysfunction risk cluster
Anticonvulsant + hormonal therapy → endocrine suppression
Multi-drug regimens → reduced ability to identify cause
Evidence
Sexual dysfunction occurs in ~50% of antipsychotic-treated patients in some cohorts due to prolactin effects
Hyperprolactinemia is strongly linked to sexual dysfunction and hypogonadism
Prolactin-raising antipsychotics (risperidone, paliperidone) have higher sexual side-effect burden
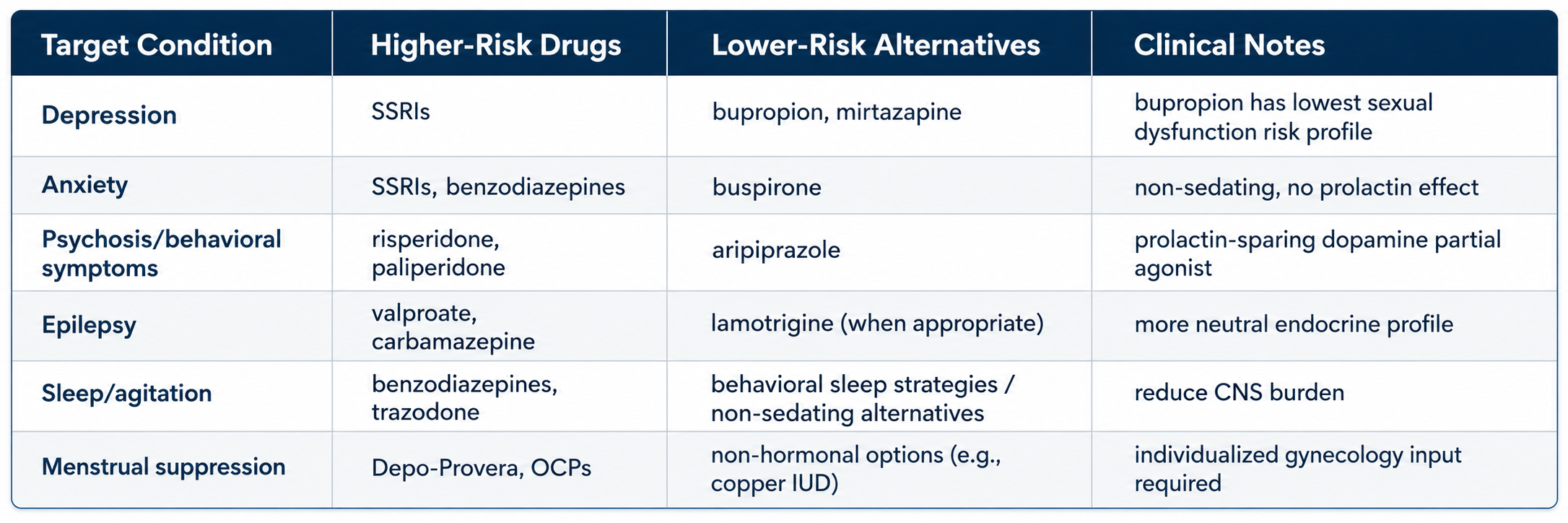
Lower Sexual Side-Effect Alternatives (IDD-Focused Substitution Options)
Key Evidence
Switching to aripiprazole reduces prolactin and sexual dysfunction risk
Guidelines recommend aripiprazole switch or augmentation for antipsychotic-induced sexual dysfunction
Bupropion shows low rates of sexual dysfunction compared with SSRIs
Aripiprazole is consistently associated with lower prolactin elevation vs risperidone/paliperidone
Clinical Issues: In women with IDD, sexual dysfunction is most often driven by combined medication burden rather than a single drug.
Highest-yield interventions
Reduce polypharmacy load (especially sedatives + antipsychotics + SSRIs)
Switch prolactin-raising antipsychotics → aripiprazole
Replace SSRIs (when clinically appropriate) → bupropion or mirtazapine
Avoid layering sedatives unless strictly necessary
Sources
National Library of Medicine – Antidepressant-associated sexual dysfunction
National Library of Medicine – Management of antidepressant sexual side effects
National Library of Medicine – Antipsychotic-induced sexual dysfunction
NCBI Bookshelf – Opioid-induced endocrine and sexual effects
Aripiprazole is consistently associated with lower prolactin elevation vs risperidone/paliperidone
In women with IDD, sexual dysfunction is most often driven by combined medication burden rather than a single drug. Highest-yield interventions:
Reduce polypharmacy load (especially sedatives + antipsychotics + SSRIs)
Switch prolactin-raising antipsychotics → aripiprazole
Replace SSRIs (when clinically appropriate) → bupropion or mirtazapine
Avoid layering sedatives unless strictly necessary
Vitamin D Issues: Low vitamin D levels have been associated with sexual dysfunction in both men and women in the general population. In men, lower vitamin D concentrations are linked to greater erectile dysfunction severity, reduced testosterone levels in some studies, and impaired endothelial function. In women, limited observational evidence suggests associations with reduced sexual desire, lower arousal, and increased sexual distress. Proposed mechanisms include effects on vascular function, hormone regulation, mood, and pelvic floor muscle function. However, most evidence is observational, and intervention studies have produced inconsistent results; therefore, a causal relationship and the effectiveness of vitamin D supplementation for improving sexual function remain unproven.
Vitamin D insufficiency is highly prevalent among people with IDD due to factors such as reduced sun exposure, institutional living, anticonvulsant use, and inadequate dietary intake and supplementation without monitoring serum levels. Although no studies have directly demonstrated that correction of vitamin D deficiency improves sexual function in IDD populations, vitamin D deficiency may contribute to sexual dysfunction alongside other common risk factors, including psychotropic medication and Depo Provera use, depression, fatigue, limited mobility, and polypharmacy. Clinically, vitamin D should be considered a potentially modifiable contributing factor rather than a primary cause of sexual dysfunction, with particular relevance in individuals receiving anticonvulsants or those with low sunlight exposure and coexisting physical or mental health concerns.
Key References
Vitamin D and erectile dysfunction association (systematic review)
Vitamin D and female sexual function studies (observational data)
Vitamin D deficiency common in epilepsy/anticonvulsant use (relevant to IDD)
About the Author

Mary Pittaway has worked in public health in state and county governments, non-profit and private organizations since the early 1970’s. During her professional career, she’s initiated and managed state and local public health programs including WIC, community sustainable agriculture start-ups, osteoporosis prevention, population-based breastfeeding work, health department accreditation, obesity prevention, community-based vitamin D interventions, farmer’s market development and population-based health promotion for people with intellectual and developmental disabilities. As a faculty affiliate at the University of Montana Department of Health and Human Performance, she teaches public health nutrition.
She filled the role of Health Promotion Global Clinical Advisor with Special Olympics International for 20 years and now consults with Special Olympics on population-based health provides Public Health consultation services for Special Olympics focusing on strategies to identify and support intentional inclusion of people with intellectual disabilities into evidence based public health programs. Mary owns and manages Diversified Resources, a small business that delivers osteoporosis prevention, screening, education, and referral services.
References
Serretti A, Chiesa A. Treatment-emergent sexual dysfunction related to antidepressants: a meta-analysis. Journal of Clinical Psychopharmacology. 2009;29(3):259–266.
Montejo ÁL, Montejo L, Navarro-Cremades F. Management strategies for antidepressant-related sexual dysfunction: a clinical approach. Journal of Clinical Medicine. 2019;8(10):1640.
National Center for Biotechnology Information. Antipsychotic-induced sexual dysfunction and hyperprolactinemia. In: StatPearls. Treasure Island, FL: StatPearls Publishing.
National Center for Biotechnology Information. Opioid-induced endocrinopathy and sexual dysfunction. In: StatPearls. Treasure Island, FL: StatPearls Publishing.
Crafa A, Cannarella R, Condorelli RA, et al. The role of vitamin D in male sexual and reproductive health: a review. International Journal of Molecular Sciences. 2020;21(21):8268